Patient Flow in Action
A talk delivered at the Whole of Health Program Masterclass, 20 May 2026, NSW Parliament House, Sydney
Before I begin, I would like to acknowledge the traditional custodians of the lands on which we meet – The Gadigal people of the Eora Nation – and to acknowledge that Indigenous Australians have poorer health outcomes and experiences than non-Indigenous Australians. Patient flow problems contribute to health inequities. I ask everyone present today to commit to doing their very best to close the gap.

Thank you for the invitation to speak today. I think this means I have been officially outed as a patient flow nerd!
I’m an emergency physician. I’m currently working in medical administration roles across Northern Sydney Local Health District, following a close encounter with cancer in 2025. I previously worked as Director of Emergency Medicine at Hornsby Ku-ring-gai Hospital. I served as President of the Australasian College for Emergency Medicine (ACEM) from 2021 to 2023. During this time, I visited more than 80 hospitals across Australia and Aotearoa New Zealand, and most of the conversations I had centred on patient flow. When you are President of ACEM, you become the official spokesperson on access block. Ministers, staffers, health departments, hospital executives, and clinical leaders, as well as journalists, all want to talk with you about patient flow problems, and to discuss potential solutions.
Conversations about access block have now moved well beyond emergency departments (EDs). I find this really encouraging. I’m sure that everyone in this room knows that while patient flow problems manifest in EDs as overcrowding and ambulance ramping, EDs themselves are not usually the root cause of the problem.
Today, I have been asked to give you some practical advice based on what I have seen and heard in my various roles. I would like to thank everyone who has shared their expertise and ideas with me over many years. I must admit that when it comes to solving patient flow, there are no shortcuts or simple solutions out there. If there were, I think we would have implemented them by now. But don’t lose heart. There are some meaningful things that we can do.
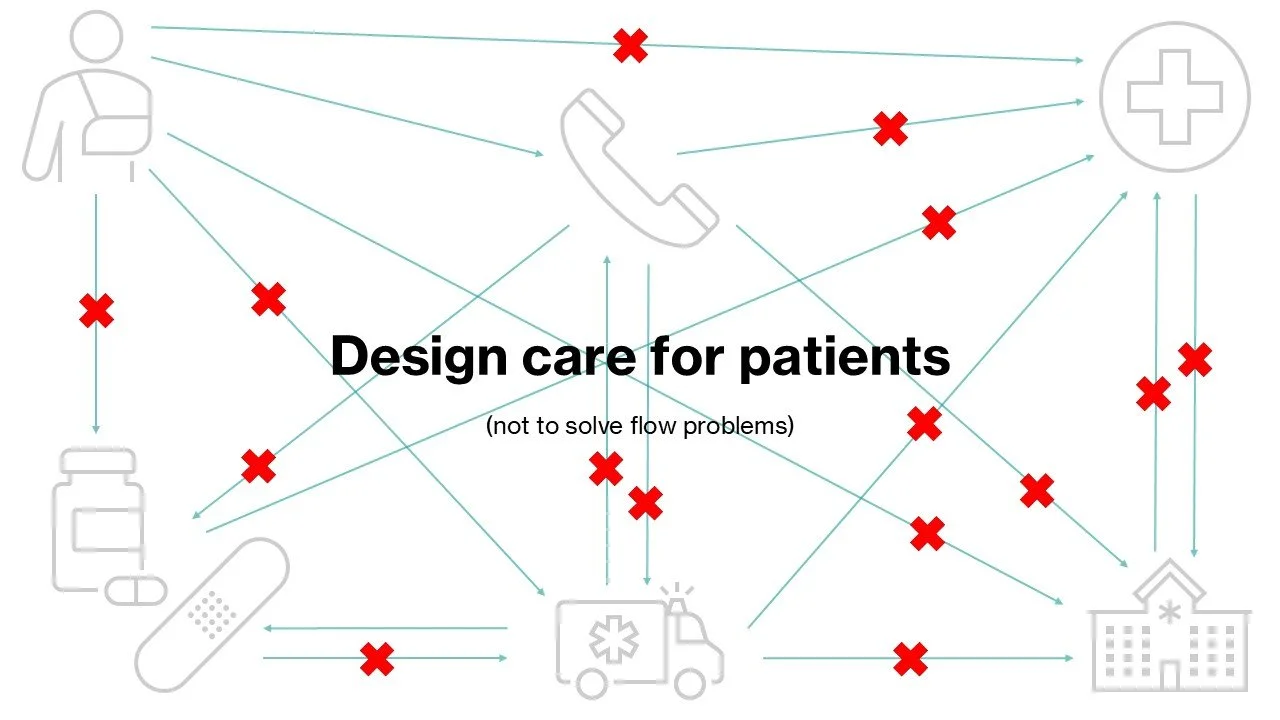
Design care for patients
Let’s start with a simple but important principle. Don’t build a new unit, or introduce a new service, with the primary goal of improving flow. Instead, design models of care that serve real patients, with real problems and needs. Otherwise, you just add complexity – more little boxes in series, or in parallel, and more opportunities for congested traffic or wrong doors – in an already overloaded patient flow circuit.
The only exception I make to this rule is for transit units, which I think can serve a genuine need for departing patients, for example a person who is waiting for a lift home from their daughter or for their discharge medications to be delivered. I’m sceptical about the use of transit units for arrivals – I’m not sure that the needs of new patients from ED, who might not be completely worked up yet, are well served by reverse transit models. I think new patients need medical and nursing expertise on appropriate inpatient wards.
Of course, there are some models of care that meet clinical needs and also improve flow. Geriatric Emergency Medicine Short Stay Units (GEMSSUs) are a great example. They give frail, elderly people improved access to senior medical decision-making and allied health advice, while minimising time spent in hospital, which we know, for this group, is associated with adverse events including delirium and falls. If you’re interested in improving outcomes for elderly patients who present to ED, have a look at the GEMSSU models in operation at Hornsby and Blacktown Hospitals.

One size does not fit all
Every health service is different. They exist in different socioeconomic contexts, with different community supports around them, and have different workforces with different skills. They inhabit different politics and serve different patients with different care needs.
It is really tempting to see a model of care that seems to work somewhere else and just transplant it into your context. It is superficially appealing to try to make everything, everywhere, the same. But that just doesn’t work. Instead, borrow the principles. Adapt them to local circumstances, then communicate about your model very clearly, and to all stakeholders, as publicly and often as possible. Monitor performance, listen to feedback, and tweak your model of care as you go.
In Australia, we love to look to the United Kingdom’s National Health Service (NHS) for guidance. I’d advise caution when trying to implement a model of care from the UK here. My colleague, Adjunct Associate Professor Peter Roberts, and I recently convened a conference about patient flow. We invited Dr Louella Vaughan, an acute physician working in London, to speak about patient flow initiatives in England. To cut a long story short, many of the NHS models don’t work. A video of her talk is available via the Good EM website, and I encourage you to watch.

Untangle the tangles and bridge the gaps
Clinicians will tell you where the friction points and discontinuities in health services are. Trust their feedback and work with them to improve and integrate care. Please don’t tell clinicians to use a new model of care – or to use an existing but dysfunctional model more – to prove that it will fail. That’s like whipping a horse until it runs across a broken bridge. When you do this, clinicians will disengage, and the model is doomed from the outset. Instead, listen carefully and incorporate their suggested changes during the design phase.
There are too many examples of well-intended services that don’t align with patient demand or clinical workflows, such as medical assessment units that can’t accept admissions from ED at times of peak presentations, or outpatient clinics with referral processes that are too difficult for patients or healthcare staff to navigate.
Professor Clair Sullivan, from Princess Alexandra Hospital in Brisbane, has done a lot of work on improving flow, communication and patient safety across care transitions. She also spoke at the Good EM patient flow conference - watch her talk here.
I dream of untangling the ED waiting room, using a concierge staff member and computer-aided decision support, a bit like the systems that have been implemented at Service NSW. Using nurse triage, and some information about past medical history and activities of daily living entered by the patient or a carer into an iPad or computer kiosk, we could stream patients according to clinical urgency (their triage score), complexity (indication for early senior doctor input), and whether they need a bed, a chair, or a cubicle to ‘see and treat’. The Patient Experience Officer could guide each patient, in order, to the next available appropriate treatment space, freeing up all the ED clinician time that goes into finding (and tidying up) a treatment area. It sounds like a fantasy – but have any of you ever checked into a private hospital for surgery? See – it can be done better.

Bring people together
And not just for operational meetings or to talk about problems. This is the secret sauce of smaller hospitals, which often work better than large ones. People know each other, feel a sense of belonging to a community, and work together to drive positive change.
Culture is like a garden. You need to water it, weed it, and make sure it gets plenty of sunshine.
Good processes are based on relationships. Foster them, across professions, teams and specialties, but with clear boundaries and roles so that people don’t burn out.
Don’t let digitised processes block real life interactions. I wrote a story about this once, after an intern described to me how it felt to be tasked by electronic messages. When I was at the start of my medical career, I knew all the nurses, because the only way to find out which jobs needed to be done was to check the book at the front desk of each ward – and have a cuppa and a chat while I was there. Please don’t just message someone. Walk the wards or pick up the phone and talk.
‘Hi Clare. It’s the bed manager. The 7B NUM asked me to call you to ask you to call the cardio reg to ask her to call her consultant to find out if the patient in bed 6 can go home today’. I’m confident that some version of this phone call plays out dozens of times each day in your hospital. In my current medical admin role, it seems that some patient flow problems might evaporate if nurses and doctors spoke with each other more. Especially if the nurse unit managers felt empowered to speak directly with the consultants about patient care.
Plan the unplanned care and smooth the planned care
It’s time to bust a myth. Unplanned hospital care is surprisingly predictable. That’s right – we know who comes through emergency departments each day, how many appendicectomies we do each week, how many chest infections we treat, and how many femurs get fractured. We should plan the unplanned care better – with emergency theatre lists, after-hours staffing, and proactive allocation of the resources we need to effectively provide that care.
Most bottlenecks in patient flow are caused by peaks and troughs in planned care. The graph that Justin presented earlier, with ambulance offload times across each weekly period looking a bit like an ECG trace of atrial flutter, demonstrates precisely that. If you’re not already aware of it, look up the work of Dr Eugene Litvak and the Institute for Health Optimisation in the USA.
Most hospitals run big surgical cases, such as spinal lists, early in the week. From the surgeon’s perspective, this probably makes sense. Those patients are most at risk of post-operative complications during the remaining days of the working week, not over the weekend. But – this practice has big knock-on effects on hospital-wide capacity. Think of the associated demand for ICU beds, follow-up diagnostic tests and social work consults. Think of the ED waiting room on Monday evenings.
We can smooth this out. Spread out elective admissions and planned surgery, and make the working day on wards more predictable, with regular consultant ward rounds, pre-assigned slots for family meetings, and carefully prioritised allied health reviews. I remember a NSW Health program from around 2005 called ‘Barbara’s Journey’ that attempted to do exactly this. I couldn’t find any trace of it left on the internet.
Timing of outpatient clinics matters too. Think about fracture clinic at your hospital. Sixty to eighty patients, all arriving at once, each needing an x-ray, most needing a splint and physiotherapy review, some needing surgery or an admission – all lumped into two or three afternoons per week. As an aside, I remember a clinical redesign project at my hospital that aimed to improve processes in our fracture clinic. It was suggested the clinic might be renamed ‘Orthopaedic Follow-Up Clinic (O.F.U.C.). Funny! That was exactly how patients felt when they saw the queue.
Redesign outpatient clinics
Outpatient clinics are ripe for reform. There are too many clinics designed around narrow diagnoses, not symptoms or syndromes, resulting in lots of wrong doors, and patients bouncing around or trapped in the system. Clinics need good administration, with senior clinician input into triage processes, and authorisation for forward referral when indicated. Clinics need realistic appointment times or they back-up – see the work of Dr Mark Mackay from South Australia, who spoke at the patient flow conference (watch his talk here). They need senior doctors present – so decisions are not just deferred to the next clinic by more junior team members – and clear criteria for referral back to primary care. Clinics need to be designed and timed so that associated services, such as diagnostic tests, allied health reviews, theatre lists and inpatient beds, can be accessed when required.
Outpatient clinics can be very useful as step down from ED or inpatient care. To work this way, they need broad inclusion criteria, simple referral processes, and senior clinician engagement. The Paediatric Acute Review Clinic at Hornsby Hospital is a fantastic service that allows a child who is borderline for needing admission to go home with close follow up by paediatric nurses and doctors, including checking pending diagnostic results. Feedback from parents is very positive. I wish we had an equivalent service for adults.
Sort the governance
This is important but not immediately obvious. Most hospitals have a divisional structure – usually medicine, surgery, and women’s and children’s health. These divisions were invented before EDs and intensive care units existed and don’t reflect current conditions. It makes more sense to group services with similar operating models, or shared patient cohorts, together. EDs have high volume and activity, and during my hospital visits, I noticed that health services with the best patient flow practices tended to have EDs represented directly in their governance structure, not buried within the division of medicine or surgery. Clinicians should be embedded in the executive, with enough non-patient-facing time remunerated to allow them to lead well. Business and project managers, with appropriate qualifications and expertise, should be embedded in clinical teams, to support clinical leaders with service planning, clinical redesign and change management.
It is important to align KPIs across the entire health service. For example, tight KPIs on diagnostic tests in ED, when there are no diagnostic KPIs on the wards, drive ED delays. If you can get a CT scan in ED in a few hours, but it takes two or three days on the ward, then inpatient teams will not accept admissions from ED unless patients are completely worked up.
The Tragedy of the Commons
I would like to thank Dr Kendall Bein, an emergency physician from Royal Prince Alfred Hospital, for devising this elegant analogy for access block.
The Tragedy of the Commons is an economic concept, describing the situation where individuals, acting in their own short-term interest, deplete a shared resource, even though it is no-one’s best interest to do so in the longer-term. Professor Elinor Ostrom won a Nobel Prize for describing a solution. People using a shared resource need to create clear boundaries and rules, monitor them, be accountable to them, and sanction individuals who don’t cooperate.
This makes sense in the hospital context. The ED represents the over-grazed commons, where patient demand backs-up when other services are overloaded. Surgeons understand patient flow, because they need available beds to operate – and planned surgery will be cancelled when beds are filled by other services. Paediatricians also manage flow relatively well because they can only admit patients to beds on designated children’s wards. Maybe we need to get back to home wards? Or, at least, very deliberately allocate a numeric or geographic bed base to each inpatient medical team?
Access to senior decision-makers
Lack of timely access to senior decision-makers, especially consultant doctors, is a major problem that creates duplication and delays. Access to senior decision-makers is hampered by clinical hierarchies and competing priorities. The on-call gastroenterologist might be busy doing a scope. The orthopaedic registrar is in clinic. The mental health clinical nurse consultant has to wait to talk to the psychiatry registrar who has to review the patient himself before speaking with the consultant psychiatrist.
There are potential economies of scale to be achieved from running an on-call roster for senior clinical input at regional, or even statewide, level – with specialists employed to be available to give immediate advice by phone or video call, not busy in their rooms or doing other things. We are seeing this sort of model emerge in services like vCare in regional NSW, the WA Country Health Service, or the Patient Access Coordination Hubs across Queensland.
Some medical specialty teams have moved to team-based care, for example the renal unit at Royal North Shore Hospital, or neurology at Hornsby – and intensive care at every major hospital in Australia. The on-call consultant rounds on all inpatients, regardless of who was on call when the patient was admitted. They are rostered to do this in a predictable pattern and move other commitments to be available for hospital care. This model also makes life much simpler for registrars, residents and interns, who do not have to work around multiple consultant rounds each day.
Patient flow initiatives need to ask the right questions of the right people. There is no point asking an intern when a patient will be discharged because they don’t have enough experience to know yet. You need senior medical engagement to make a difference – and that might mean running or timing meetings about patient flow differently.
A word of caution. You need to be mindful of providing teaching and learning opportunities for clinicians in training. Most health professions still follow an apprenticeship model. While you need senior clinicians to make decisions, you need to make sure that junior clinicians are not cut out of the loop entirely. They need to learn how and why clinical decisions are made.

Money matters
Too often, clinical redesign projects fail because money is not considered at all, or because financial analysis lacks sophistication. The way we fund healthcare in Australia is exceptionally complicated. Activity-based vs block vs historic funding. Medicare and the pharmaceutical benefits scheme. Private health insurance. Out-of-pocket costs for patients and carers. Commonwealth vs state vs local government responsibilities.
Clinical leaders need to be across health finance and economics. In particular, they need to understand opportunity cost and moral hazard.
At clinical unit level, we tend to save pennies to spend pounds. We don’t employ enough staff to cover planned and unplanned leave, so costs blow out on premium labour. We don’t have enough working equipment. Walk into any ED during the afternoon shift and mentally calculate how much hospitals pay clinicians to queue up to use a computer.
When it comes to patient flow, how doctors are paid really matters. Some doctors earn a salary. Some are paid by the session. Others are paid fee-for-service – they only receive payment when they see a patient admitted under their own card in a hospital bed. Most patient flow initiatives fundamentally misunderstand how doctors work and how they earn an income. I think this topic deserves a separate talk on another day – perhaps at a future Whole of Health Program workshop?

Less is more
Have you read the paper ‘Getting Rid of Stupid Stuff?’ It is my favourite ever article from the New England Journal of Medicine.
There is a lot of work as imagined happening in hospital board room discussions. Work as imagined is very different from work as done. If you haven’t already, explore the writings of Dr Steven Shorrock on his Humanistic Systems website. So much energy goes into working around prescribed processes that don’t work well. Associate Professor Nick Taylor, an emergency physician from Canberra, gave an insightful talk about normalisation of deviance in healthcare at the ACEM conference a few years ago. When the prescribed way of doing something is clunky, busy clinicians devise shortcuts. When those deviations seem to work, or don’t result in visible harm, further short cuts are taken. Clinical practice drifts progressively further from guidelines and evidence, eventually impacting patient and clinician safety.
The first step of a clinical redesign project is to map the service. The second step should be simplification – removing every unnecessary step. Getting rid of stupid stuff.
Please trust and respect clinicians who provide challenging feedback. Don’t just assume they are being difficult or are resistant to change. Find out what they know and use that information to design better and safer ways of getting things done.
Be mindful of the work pressures healthcare professionals are under. Beware allocating even minor administrative tasks to clinicians. ‘It will only take a few minutes’ becomes hours when multiplied across many patients per day.
Tread gently with unwritten rules that have arisen from adverse outcomes. Every hospital has odd things that spook people. Clinicians have long memories and deep emotional ties to past patients. Trust is important. If something doesn’t make sense to you, please ask why it is done that way, and be very sensitive and careful with how you negotiate change.
Nagging doesn’t work
I want you all to reflect on a time when nagging made you change your mind or do something you didn’t want to do. See! It really doesn’t work. Instead, ask how you can help.
Negative feedback doesn’t work very well either. Shame is a negative motivator.
I still remember the time when a hospital executive called me to complain about a small drop in one rating on the Bureau of Health Information patient experience survey. That was the year that Hornsby ED was on the front page of the Sydney Morning Herald for topping the state.
Find the positives – always. Create a shared vision of better ways of working, with patient care at the heart.
Leadership should bear witness and offer genuine support.
Don’t nag clinicians to shave off minutes in a single patient’s journey. Do the deep structural work required to free up hours or days for everyone – patients, carers, and clinicians.
Digital done well
I know you know this, but the data dashboard does not tell the full story. The map is not the territory.
The ED navigator does not need you to look at the portal and call to tell her that there is an ambulance that needs offloading. She knows. She’s there. She can see it. Get down to ED and have a look around. Listen. Help. Don’t just document that you made a call.
These days, it is easy to create digital tools. We have a data display or checklist for almost every aspect of patient care. But pages of static information are no longer enough. To be useful, digital tools must predict problems and facilitate their prevention, and be highly focused. We need to think of the clinician user experience – every alert creates a risk of diversion or distraction from a more critical task. We also need to think of the patient and carer experience – do digital tools reflect what matters to them?
The big picture
At the start, I said there is no simple fix for patient flow. Here are some big picture things we need to do.
We need enough capacity in hospitals. For now. Not for some perfect, predicted future state.
We need to fix primary and community care – especially aged, disability and mental health care. That is likely to require some investment in residential and semi-residential or drop-in models. We need to empower general practice. I would love a local health district to partner with a primary health network to build a wrap-around health ecosystem using pooled commonwealth, state and local funding. We have some new hospitals coming online in New South Wales that might present this opportunity.
We need to invest in innovation. Not just band aids and cute projects. Not hoping we will drive change through slashing budgets. We need to genuinely reimagine care systems with resources, expertise and care.
Patient flow is a wicked problem. It’s complex. Hospitals don’t work like freeways or factory production lines. Assistant Professor Kieran Le Plastrier, an academic General Practitioner, spoke about this at the patient flow conference – watch his talk here. To fix patient flow, we need to learn about complexity science and look to soft systems methodology for meaningful solutions.
Patient flow is not easy, but it’s really important – for patients and healthcare staff. If we work together, we can make a difference.
Thank you for the opportunity to speak with you today.
Dr Clare Skinner is a specialist emergency physician, communicator and health reform strategist. She is former President of the Australasian College for Emergency Medicine and works as a clinician, educator and health executive. Clare has special interests in clinical leadership, governance and workplace culture. She is deeply committed to improving population health using an inclusive, person-centred and evidence-informed approach. Clare was selected in the Top 50 Public Sector Women NSW in 2018.